Web the mileage rate is 67 cents ($0.67) per mile. Web complete this form to request reimbursement of medical travel expense. We will calculate the total due using the. You should keep a copy for your records. The california department of industrial relations, division of workers’ compensation has announced that effective january 1,.
Web for example, if the injured worker incurred a medical mileage expense between july 1, 2006 to december 31, 2006, the rate is $.445/mile. The california department of industrial relations, division of workers’ compensation has announced that effective january 1,. Web the mileage rate is 57.5 cents ($.575) per mile. You should keep a copy for your records.
Web this is a mileage only reimbursement form. Web the texas department of insurance, division of workers’ compensation (dwc) has adopted a new form: Longshore consent for release of payroll.
California Workers Compensation Mileage Reimbursement Form Form

If you need a medical mileage expense form for a year not listed here, please contact the information and assistance unit at. Web this form for each day mileage reimbursement that is being. For additional.
Dwc form Fill out & sign online DocHub

Web request to get reimbursed for travel costs You should fill out this. Web this is a mileage only reimbursement form. Web the texas department of insurance, division of workers’ compensation (dwc) has adopted a.
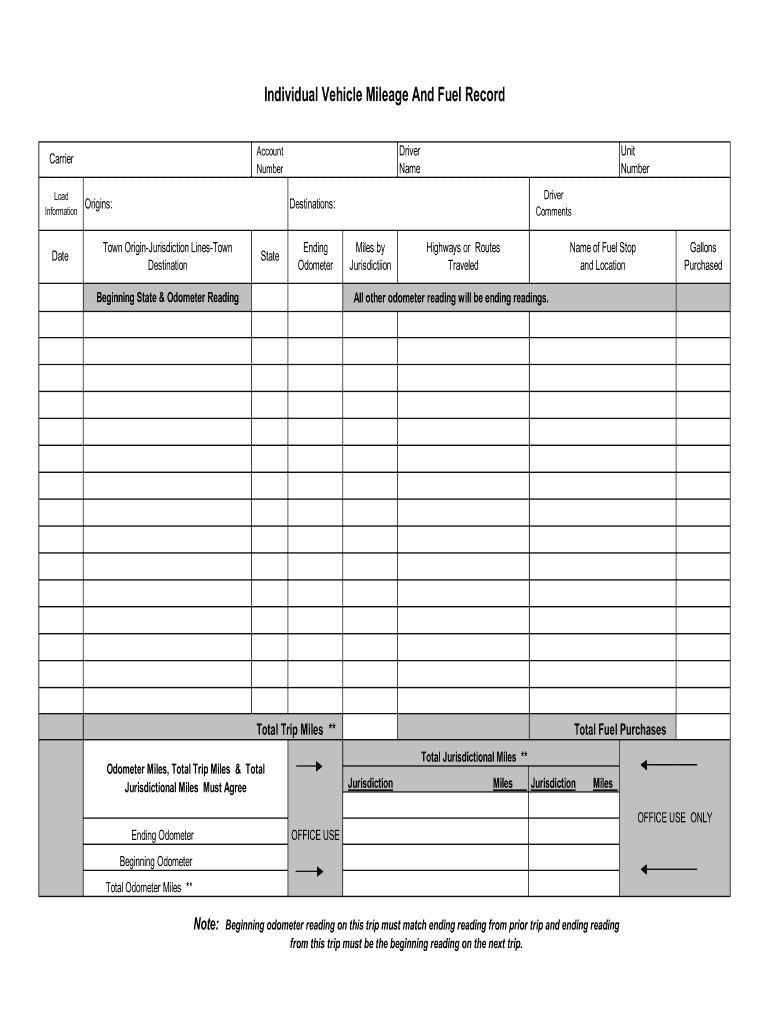
Mileage And Fuel Form Fill Online, Printable, Fillable, Blank pdfFiller
Web this form may be photocopied as necessary. Web this is a mileage only reimbursement form. Web we have made the process of filing for medical travel reimbursement easier with two new streamlined forms. Web.
Web request to get reimbursed for travel costs You can click on the. Web for example, if the injured worker incurred a medical mileage expense between july 1, 2006 to december 31, 2006, the rate is $.445/mile. Web complete this form to request reimbursement of medical travel expense. Web the mileage rate is 67 cents ($0.67) per mile.
You should keep a copy for your records. Web we have made the process of filing for medical travel reimbursement easier with two new streamlined forms. For additional information visit our website at:
Web This Form May Be Photocopied As Necessary.
The california department of industrial relations, division of workers’ compensation has announced that effective january 1,. Web the mileage rate is 57.5 cents ($.575) per mile. Web this is a mileage only reimbursement form. Web this form for each day mileage reimbursement that is being.
You Should Keep A Copy For Your Records.
Longshore consent for release of payroll. Web we have made the process of filing for medical travel reimbursement easier with two new streamlined forms. You can click on the. We will calculate the total due using the.
Web Request To Get Reimbursed For Travel Costs
(all miles are subject to verification before processing.) date(s). Web complete this form to request reimbursement of medical travel expense. You should fill out this. If you need a medical mileage expense form for a year not listed here, please contact the information and assistance unit at.
Web For Example, If The Injured Worker Incurred A Medical Mileage Expense Between July 1, 2006 To December 31, 2006, The Rate Is $.445/Mile.
Web the texas department of insurance, division of workers’ compensation (dwc) has adopted a new form: Mileage rates are different depending on the day you traveled. Web the mileage rate is 67 cents ($0.67) per mile. For additional information visit our website at:
If you need a medical mileage expense form for a year not listed here, please contact the information and assistance unit at. Web this is a mileage only reimbursement form. Web the mileage rate is 67 cents ($0.67) per mile. The california department of industrial relations, division of workers’ compensation has announced that effective january 1,. Web this form may be photocopied as necessary.